Total laryngectomy, performed for advanced disease, has been replaced by less radical resections in many cases. Hemilaryngectomy {hemilaryngectomy.jpg} is excision of either the right or left larynx with the overlying thyroid cartilage. This is indicated for early glottic lesions. The resection includes true and false cords and thyroid cartilage along with paraglottic space. We often receive modified partial laryngectomies that are customized to the patient's disease, including supraglottic specimens. To understand these, it is useful to understand some relevant anatomy.
Larynx[]
Anterior limit: composed of the anterior or lingual surface of the suprahyoid epiglotts, the thyroid membrane, the anterior commissure, and the anterior wall of the subglottic region (thyroid cartlage, cricothyroid membrane and the anterior arch of the cricoid cartilage).
Posterior and lateral limits: include the laryngeal aspect of the aryepiglottic folds, the arytenoid region and interarytenoid space, and the posterior surface of the subglottic space (mucous membrane covering the cricoid cartilage).
Superolateral limit: tip and lateral borders of the epiglottis.
Inferior limit: plane passing through the inferior edge of the cricoid cartilage.
Supraglottis[]
Composed of the epiglottis (both lingual and laryngeal aspects), aryepiglottic fold (laryngeal aspect), arytenoids, and ventricular bands (false cords).
The epiglottis can be further divided into the suprahyoid and infrahyoid portions for staging purposes.
Inferior boundary is a horizontal plane passing through the lateral margin of the ventricle at its junction with the superior surface of the vocal cord.
Glottis[]
Composed of the true vocal cords, including the anterior and posterior commissures, superior and inferior surfaces.
Occupies a horizontal plane 1 cm in thickness, extending inferior from the lateral margin of the ventricle.
Subglottis[]
Extends from the lower boundary of the glottis (1 cm below the true cords) to the lower margin of the cricoid cartilage.
Preepiglottic space[]
A deep tissue plane, lying between the mucosa and the supporting skeleton of the larynx, largely consisting of adipose tissue.
This deep tissue space is superiorly bordered by the hyoepiglottic ligament.
Anteriorly it is bordered by the thyroid cartilage, thyrohyoid membrane and cricothyroid membrane.
The posterior border consists of the epiglottis, quadrangular membrane and the anterior reflection of the pyriform sinus mucosa.
Its inferior border is formed by the conus elasticus.
Paraglottic space[]
The lateral part of the deep laryngeal tissue plane (between the laryngeal framework and the mucosa).
The paired paraglottic spaces are lateral to the pre epiglottic space.
At the level of the glottis, the paraglottic space is limited to a narrow band of fatty tissue lateral to the thyroarytenoid musle, continuous with the supraglottic submucosal fat. This deep fat plane at the level of the true vocal cord continues inferiorly as a thin infraglottic fat plane, bordered by the conus elasticus.
The line of resection in a supraglottic laryngectomy goes through the laryngeal ventricles, between the true and false vocal cords.
If a supraglottic cancer spreads inferiorly along the ventricle, in the paraglottic space at the level of the true vocal cord, then speech conservation surgery will not be possible
Fresh handling[]
Partial laryngectomy[]
Most of these specimens will be oriented by the surgeon. You must be very sure of the orientation before cutting these specimens as the anatomy will be impossible to reconstruct later. If in doubt, ask for help from your attending.
It is good practice to photograph the oriented specimen. Make a printout of the photo.
Once you have sufficient information about the specimen, it can be fixed in formalin.
Total laryngectomy[]
These specimens will usually be oriented and inked by the surgeon. If in doubt, contact him. He may not ink the mucosal margins, so you will need to ink these yourself using a new color. If he does not ink the specimen at all, at a minimum, ink the entire outside of the specimen black and place another color at the tracheal resection margin.
After the specimen is inked, it should be opened longitudinally along the posterior side using heavy scissors. It can be propped open using applicator sticks to make visualization easier later on. If tumor is large, take some for tissue banking, then fix the specimen in formalin.
Grossing in[]
Smaller specimen (small partial laryngectomy)[]
Some partial laryngectomies are small enough to submit entirely in 10 cassettes or less. For specimens like this, submitting in toto will give you the best reconstruction of the case when reviewing with your attending.
Photograph the specimen.
Ensure that margins are adequately inked. Insufficient ink will make the case difficult to sign out.
Find the lesion and describe in two dimensions. Describe color, size, quality (exophytic, flat, verrucous, ulcerated, necrotic), location, and extent of involvement of anatomic landmarks (e.g., vocal folds, ventricle, epiglottis, commissures, across midline).
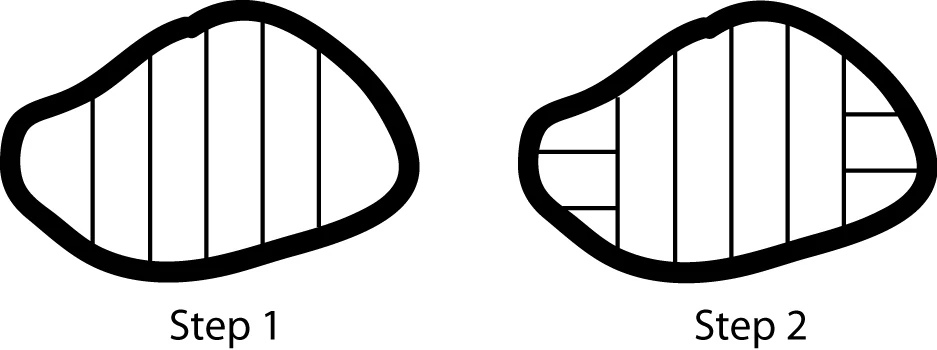
Make longitudinal cross-sections through the specimen in order to measure the third dimension of the tumor and estimate extent of invasion (into submucosa, into cartilage, through cartilage).
Submit entirely, in a way you will be able to reconstruct later (for example, proceeding from medial to lateral). It may be useful to draw your sections on a printout of the specimen photograph.
The first and last sections should be sectioned and submitted perpendicular to the
Perpendicular tips
principal axis, if there are margins to demonstrate in these areas. See diagram.
Larger specimen (hemilaryngectomy or total laryngectomy)[]
Larger partial laryngectomy specimens and total laryngectomies will have to be selectively submitted. They may contain bone (hyoid) or ossified cartilage. You will therefore need to be somewhat invasive in processing them.
Find the lesion and describe in two dimensions. Describe the lesion including color, size, quality (exophytic, flat, verrucous, ulcerated, necrotic), location, and extent of involvement of anatomic landmarks (e.g., vocal folds, ventricle, epiglottis, commissures, across midline).
Find the hyoid bone. If grossly distant from tumor, you can dissect it off and handle it separately. If it seems to be involved by tumor, you will need to leave it on the specimen.
Make longitudinal cross-sections through the specimen in order to measure the third dimension of the tumor and estimate extent of invasion (into submucosa, into cartilage, through cartilage). A large knife and mallet are often required. Don’t hesitate to ask for help.
Take sections (see diagram)
Laryngectomy sections
. The following items should be sampled for every case. But remember, one section can show multiple sites, so the total number of slides will be less than the number of sites that need to be evaluated histologically.
Tumor showing deepest level of invasion with relationship to adjacent structures (usually 4 sections):
Tumor in relationship to deepest level of invasion
Tumor in relation to paraglottic space
Tumor in relation to pre-epiglottic space
Tumor in relationship to adjacent normal mucosa to show precursor lesion
At least one rep sec of the closest soft tissue margin, which will usually be a shave or perpendicular block of the anterior radial margin (use judgment based on tumor extension).
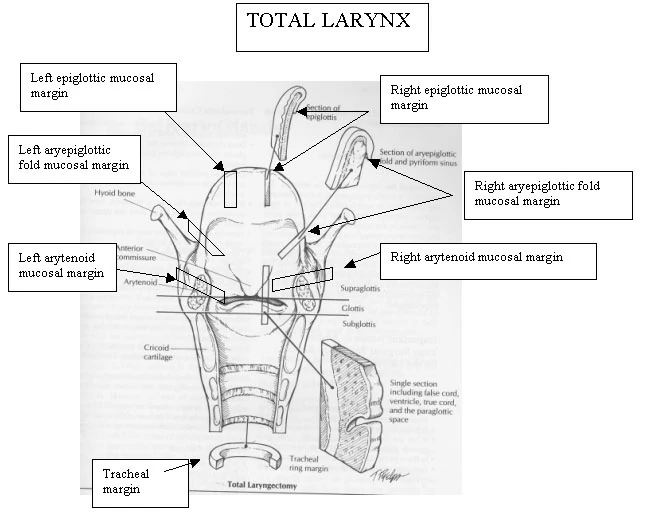
Mucosal margins; several will be present, depending on extent of resection:
Total laryngectomy will have:
Left aryepiglottic fold, left epiglottic, left arytenoid
Right aryepiglottic fold, right epiglottic, right arytenoid
Hemilaryngectomy will have either the left or the right set of mucosal margins, plus two medial mucosal margins where the larynx was divided in two—these margins are adjacent to the half of the larynx that is still in the patient.
All will have a tracheal margin (take a circumferential shave).
Sample margins closest to the tumor most extensively. All margins taken as perpendicular sections.
Some specimens will have other designated margins or will lack some of these. Just follow the surgeon’s designations.
Sample dictation[]
The specimen consists of a (total, partial) laryngectomy (___ x ___ x ___ cm), including hyoid bone and larynx from epiglottis to subglottis. The specimen is inked and oriented by the surgeon as follows: (describe). There is an irregular tan-white mass (___ x ___ x ___ cm), with central ulceration, located in the glottis, completely involving the left true vocal cord. The mass crosses the midline and involves the medial aspect of the right true vocal cord. The false vocal cords are not involved. The mass is 2.8 cm from the closest proximal mucosal margin (left aryepiglottic fold) and 5 cm from the distal tracheal margin. The mass invades in to the lamina propria and focally appears to invade into, but not through, the thyroid cartilage. The anterior surface is covered by red-brown muscle which is grossly unremarkable. 0.5 cm from the distal margin there is a 1.5 x 1 cm trachostomy. Sections are submitted as follows: (list)
Review and signout[]
Retrieve the patient’s biopsy, if available. Familiarize yourself with the definitions of the paraglottic and preepiglottic spaces so that you can determine if these are involved.
A. Invasive squamous cell carcinoma, X cm, (well, moderately, poorly) differentiated, (non) keratinizing, involving the (right/left glottis vs. supraglottis vs. subglottis vs. other location) to a depth of Y cm (with extension across the midline), (perineural invasion present), smd(F9).
B. Tracheal, laryngeal, mucosal, and anterior soft tissue margins free of involvement.
C. Tracheostomy site with skin.
D. Thyroid, no tumor identified.
E. Parathyroid, no tumor identified.
F. X lymph nodes, no tumor seen (0/X).
In the microscopic description, include a template for laryngeal cancer.
References[]
Sample dictation adapted from Lester, Manual of Surgical Pathology, 2nd ed., 2006.
Paraglottic and preepiglottic space definitions: http://www.medcyclopedia.com.

{kind=link}
{kind=link}